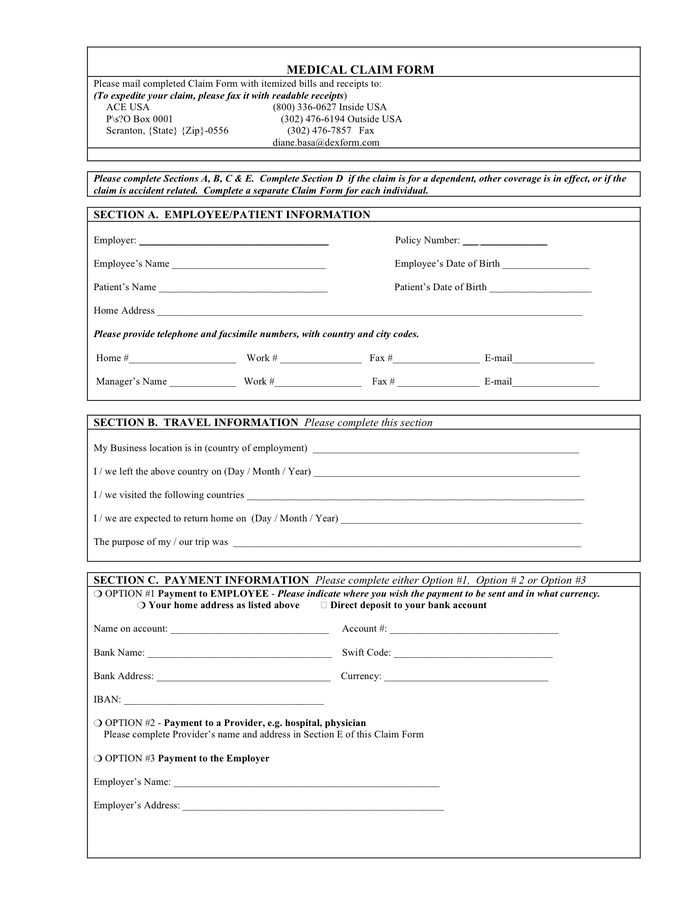
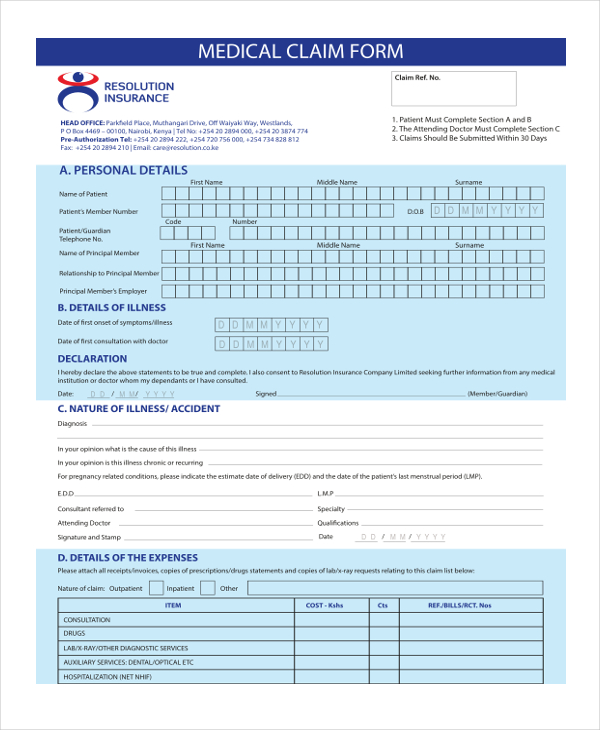
Medical Claim Form Pdf - Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Save time with easy filling and. A patient’s signature requests that payment be made and authorizes release of any information necessary. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Download the blank form in pdf and word formats. Medical claim form what is this form for?
A patient’s signature requests that payment be made and authorizes release of any information necessary. Medical claim form what is this form for? Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Download the blank form in pdf and word formats. Save time with easy filling and. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim.
Download the blank form in pdf and word formats. A patient’s signature requests that payment be made and authorizes release of any information necessary. Medical claim form what is this form for? Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Save time with easy filling and.

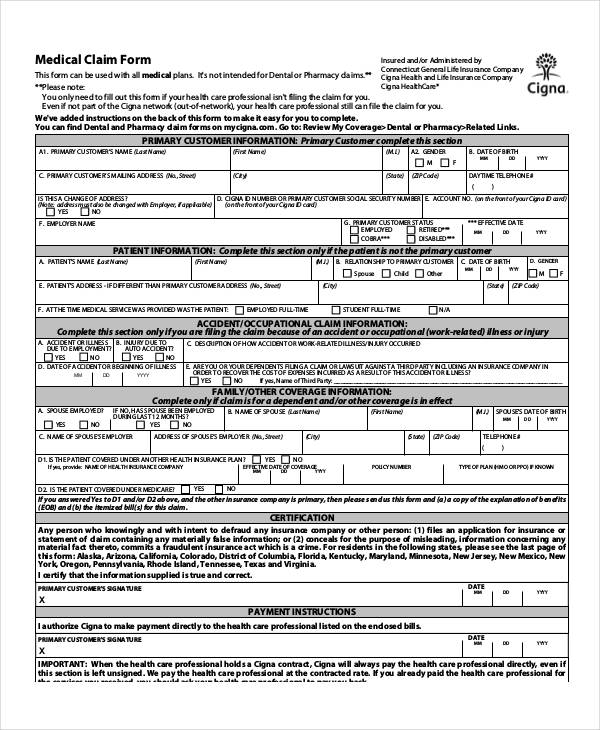
Medical Claim Form download free documents for PDF, Word and Excel
A patient’s signature requests that payment be made and authorizes release of any information necessary. Download the blank form in pdf and word formats. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Save time with easy filling and. Fill out this form if you’re asking for reimbursement of.

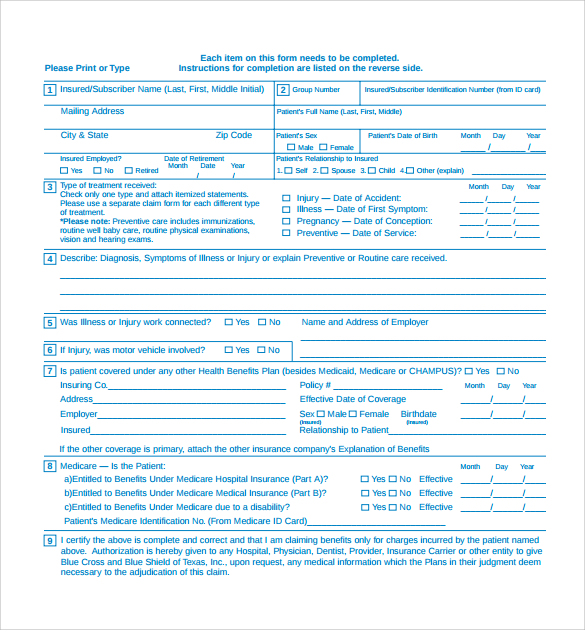
Medical Claim Form in Word and Pdf formats
A patient’s signature requests that payment be made and authorizes release of any information necessary. Download the blank form in pdf and word formats. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Save time with easy filling and. Medical claim form what is this form for?
Medical claim form in Word and Pdf formats
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Download the blank form in pdf and word formats. A patient’s signature requests that payment be made and authorizes release of any information necessary. Save time with easy filling and. Patient’s or authorized person’s signature i authorize.
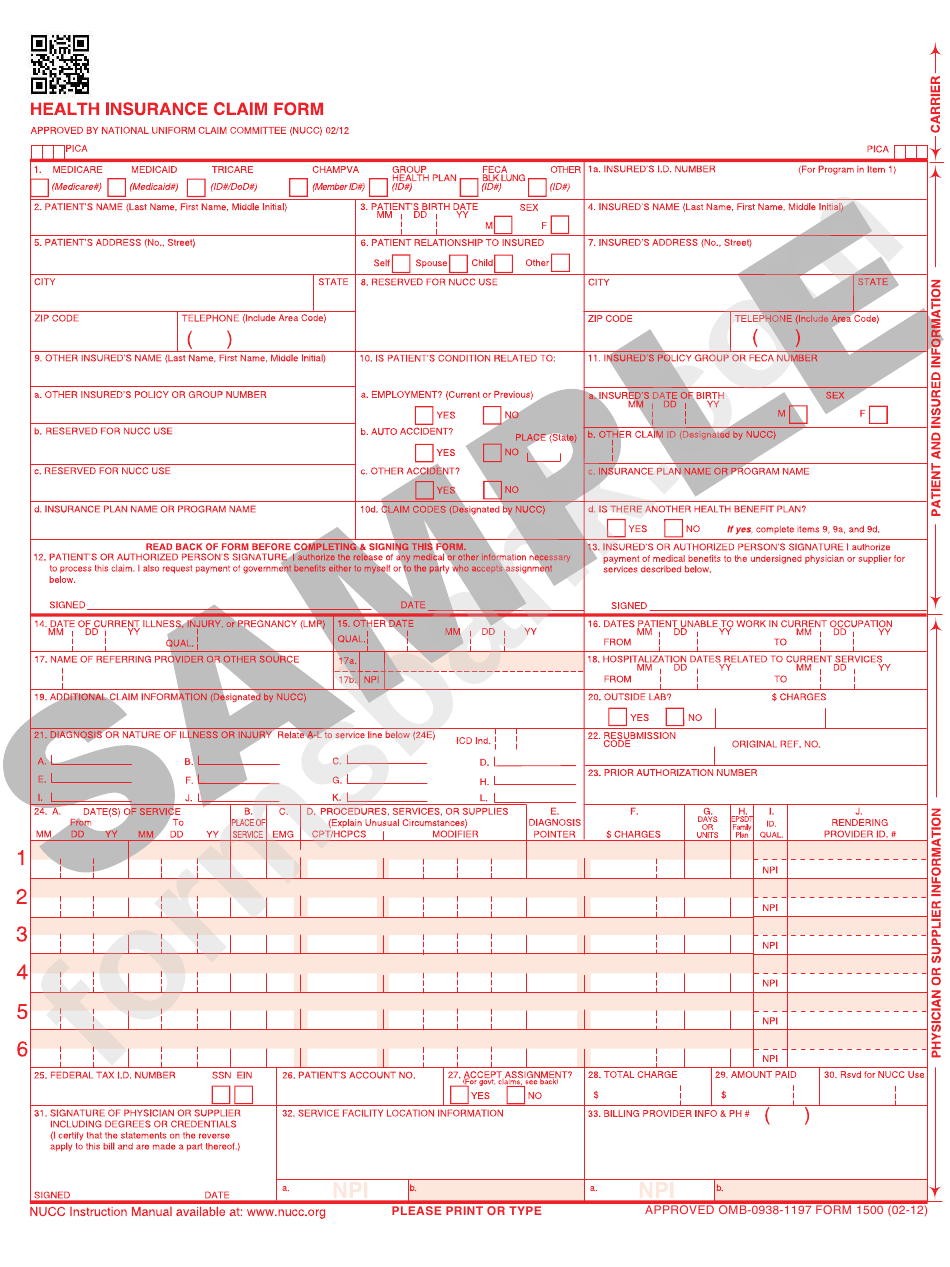
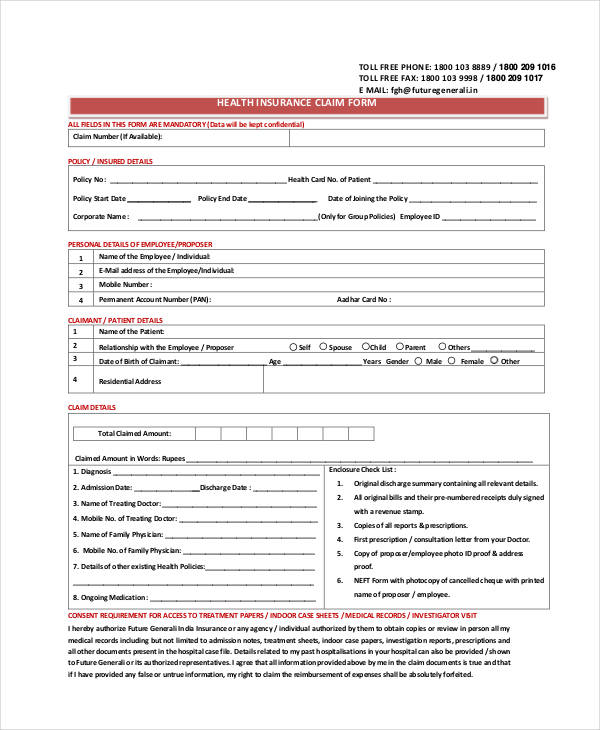
Health Insurance Claim Form printable pdf download
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Save time with easy filling and. A patient’s signature requests that payment be made and authorizes release of any information necessary. Download the blank form in pdf and word formats. Medical claim form what is this form.
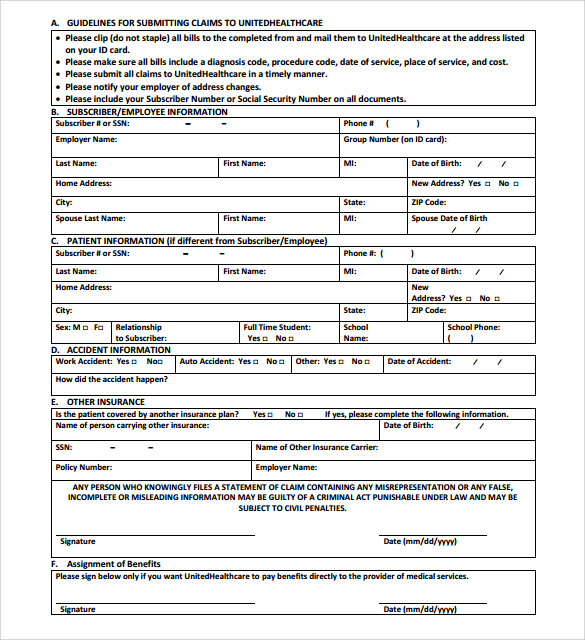
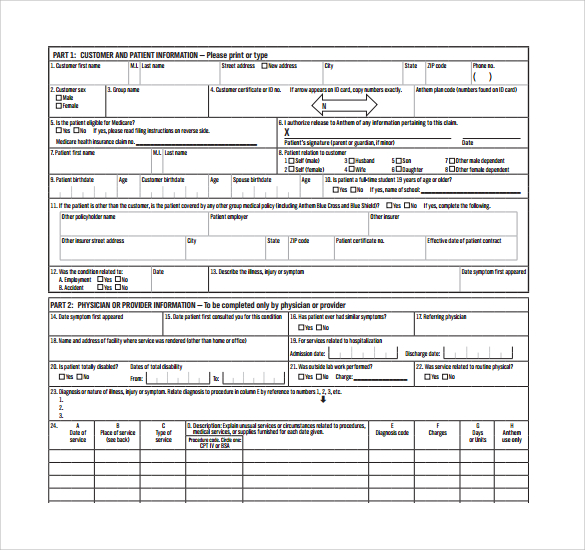
FREE 6+ Sample Medical Claim Forms in PDF
A patient’s signature requests that payment be made and authorizes release of any information necessary. Download the blank form in pdf and word formats. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Patient’s or authorized person’s signature i authorize the release of any medical or.
FREE 40+ Claim Forms in PDF Excel MS Word
Medical claim form what is this form for? Download the blank form in pdf and word formats. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Save time with easy filling and. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service,.
FREE 36+ Claim Form Samples, PDF, MS Word, Google Docs, Excel
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. A patient’s signature requests that payment be made and authorizes release of any information necessary. Save time with easy filling and. Medical claim form what is this form for? Patient’s or authorized person’s signature i authorize the.
FREE 14+ Medical Claim Forms in PDF MS Word
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Medical claim form what is this form for? Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Download the blank form in pdf and word formats..
FREE 26+ Medical Form Samples, PDF, MS Word, Google Docs, Excel
Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. A patient’s signature requests that payment be made and authorizes release of any information necessary. Download the blank form in pdf and word formats. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental.
FREE 14+ Medical Claim Forms in PDF MS Word
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Download the blank form in pdf and word formats. Save time with easy filling and. Medical claim form what is this form for? A patient’s signature requests that payment be made and authorizes release of any information.
Medical Claim Form What Is This Form For?
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Download the blank form in pdf and word formats. A patient’s signature requests that payment be made and authorizes release of any information necessary. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim.