Gainwell Pa Form - List the ndc, name, dosage form, and quantity (qty) of each ingredient. Begin the list with the. Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Each ingredient used in the compound must be listed. Request for rx prior authorization to be used for hepatitis c medication pa requests Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio.
Request for rx prior authorization to be used for hepatitis c medication pa requests Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Begin the list with the. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Each ingredient used in the compound must be listed.
Begin the list with the. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Request for rx prior authorization to be used for hepatitis c medication pa requests Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Each ingredient used in the compound must be listed.
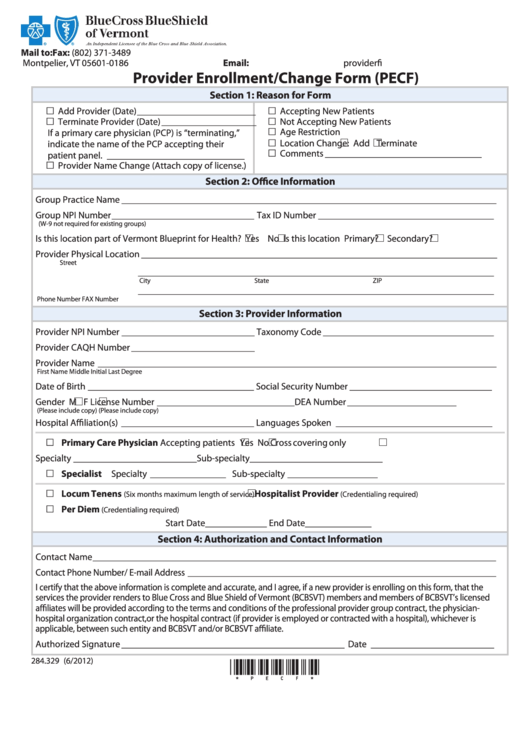
Healthy Blue Provider Enrollment Form Enrollment Form
Begin the list with the. Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Each ingredient used in the compound must be listed. List the ndc, name, dosage form,.
Capital Blue Cross Pennsylvania Prior Authorization Your Complete Guide
Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Begin the list with the. Each ingredient used in the compound must be listed. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be.
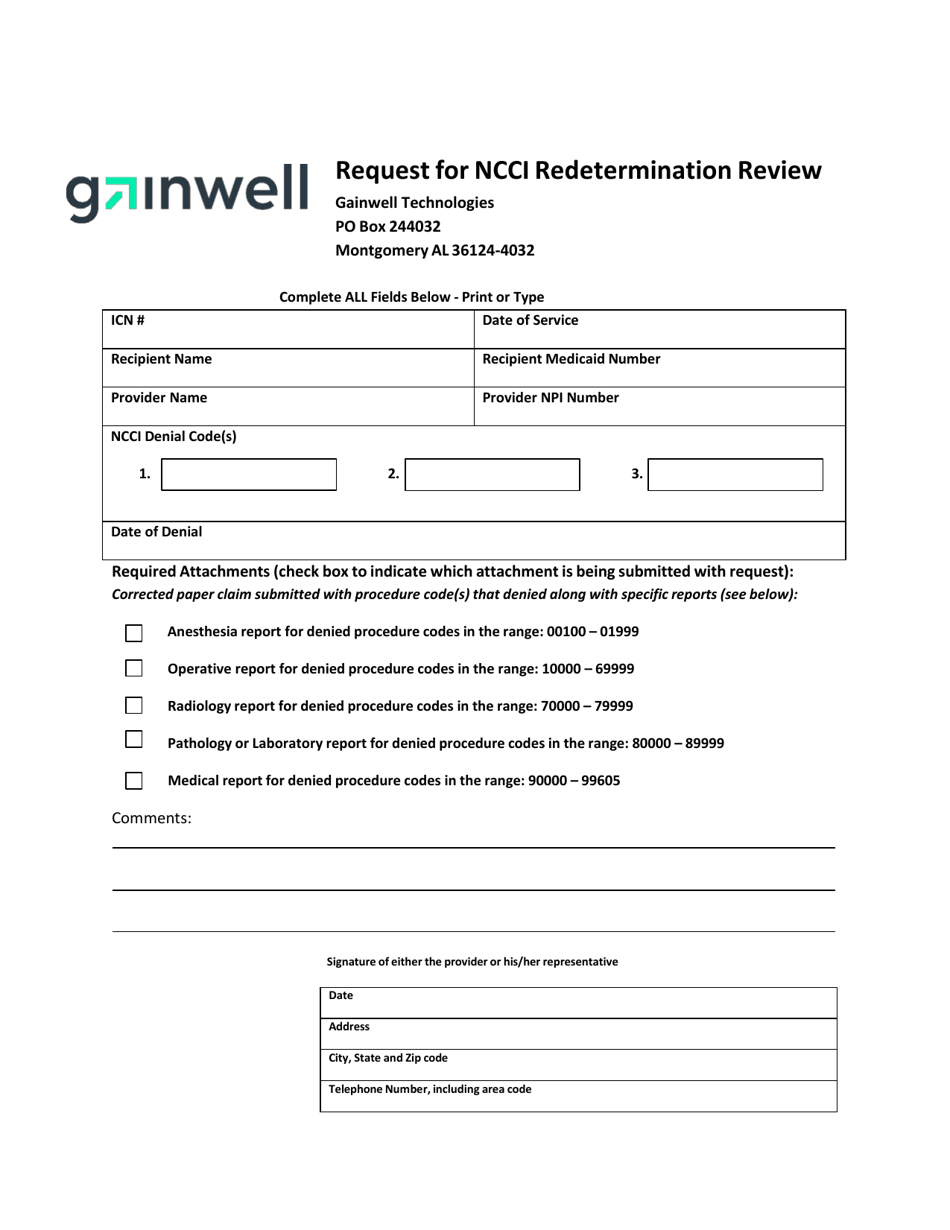
Alabama Gainwell Request for Ncci Redetermination Review Fill Out
List the ndc, name, dosage form, and quantity (qty) of each ingredient. Request for rx prior authorization to be used for hepatitis c medication pa requests Begin the list with the. Each ingredient used in the compound must be listed. Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted.
FREE 41+ Authorization Forms in PDF Excel MS word
Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Each ingredient used in the compound must be listed. Begin the list with the. Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Request for rx prior authorization to.

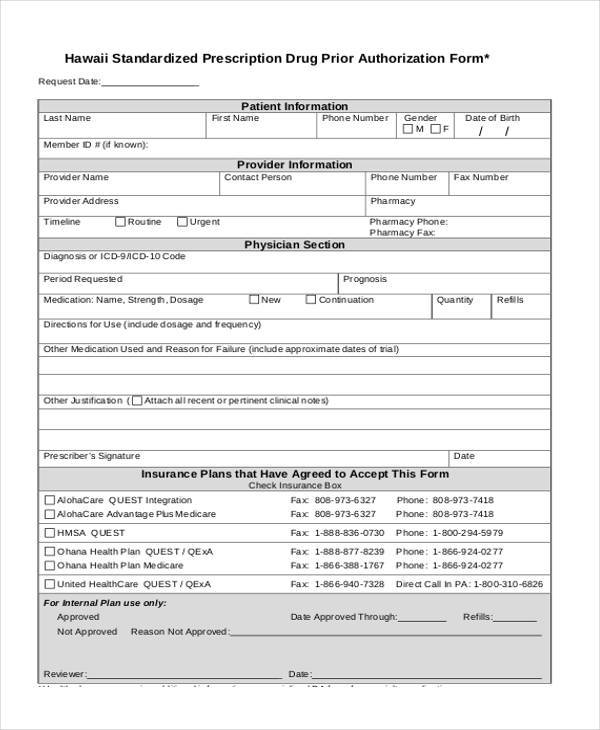
Printable Medical Prior Authorization Form Template
Each ingredient used in the compound must be listed. Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Begin the list with the. Request for rx prior authorization to.

Fillable Online medicaid ms Gainwell prior authorization form pdf
Each ingredient used in the compound must be listed. Begin the list with the. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Request for rx prior authorization to be used for hepatitis c medication pa requests Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted.
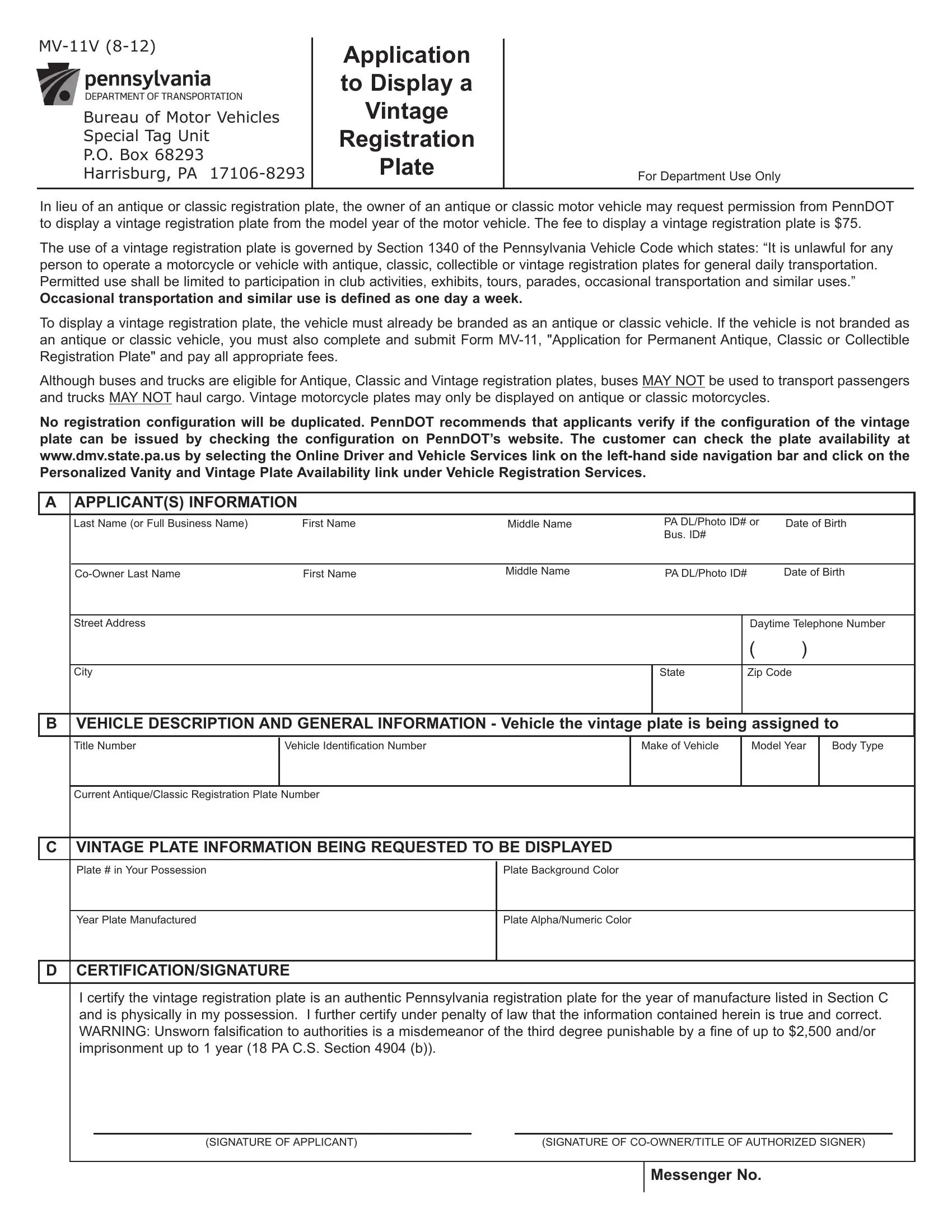
PA Form MV11V ≡ Fill Out Printable PDF Forms Online
Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. Begin the list with the. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Request for rx prior authorization to be used for hepatitis c medication pa requests Medicaid managed care plans amerihealth caritas ohio anthem blue.

Fillable Online medicaid ms Gainwell forms Fax Email Print pdfFiller
Request for rx prior authorization to be used for hepatitis c medication pa requests Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health.

How To Fill Out Ohio Medicaid Claim Form
Requests for oral medication assisted treatment (mat) for opioid use disorder (oud) should be submitted on the oral medication assisted. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Request for rx prior authorization to be used for hepatitis c medication pa requests Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health.
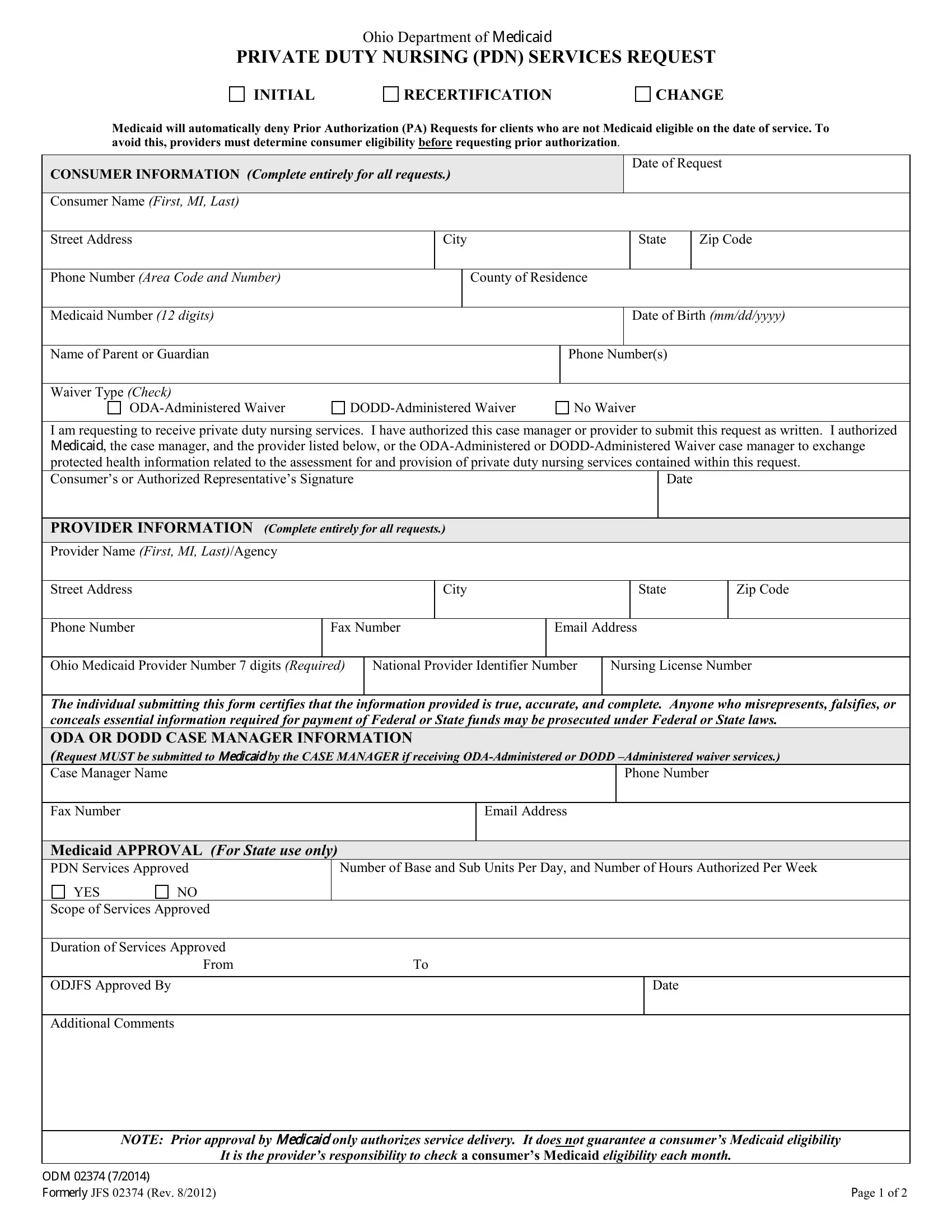
Ohio Form Odm 02374 ≡ Fill Out Printable PDF Forms Online
Begin the list with the. Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio. Each ingredient used in the compound must be listed. Request for rx prior authorization to be used for hepatitis c medication pa requests List the ndc, name, dosage form, and quantity (qty) of each ingredient.
Requests For Oral Medication Assisted Treatment (Mat) For Opioid Use Disorder (Oud) Should Be Submitted On The Oral Medication Assisted.
Each ingredient used in the compound must be listed. List the ndc, name, dosage form, and quantity (qty) of each ingredient. Request for rx prior authorization to be used for hepatitis c medication pa requests Medicaid managed care plans amerihealth caritas ohio anthem blue cross blue shield buckeye health plan caresource humana healthy horizons ohio.