Dupixent Enrollment Form - Please provide us with your email address to receive email communications. Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support program and start. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Choose the appropriate form below and complete the required fields. Start your dupixent treatment with the myway enrollment form.
Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Please provide us with your email address to receive email communications. Start your dupixent treatment with the myway enrollment form. Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support program and start. Choose the appropriate form below and complete the required fields.
Start your dupixent treatment with the myway enrollment form. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support program and start. Please provide us with your email address to receive email communications. Choose the appropriate form below and complete the required fields. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more.

DUPIXENTMyWayEnglishEnrollmentForm Medical Prescription Pharmacy
Choose the appropriate form below and complete the required fields. Start your dupixent treatment with the myway enrollment form. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Please provide us with your.

Dupixent Enrollment Form PDF Download Fillable Form Now
Please provide us with your email address to receive email communications. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. Choose the appropriate form below and complete the required fields. Start your dupixent treatment with the myway enrollment form. If i am completing section 5b, i authorize for my commercially insured patient one or more months of.
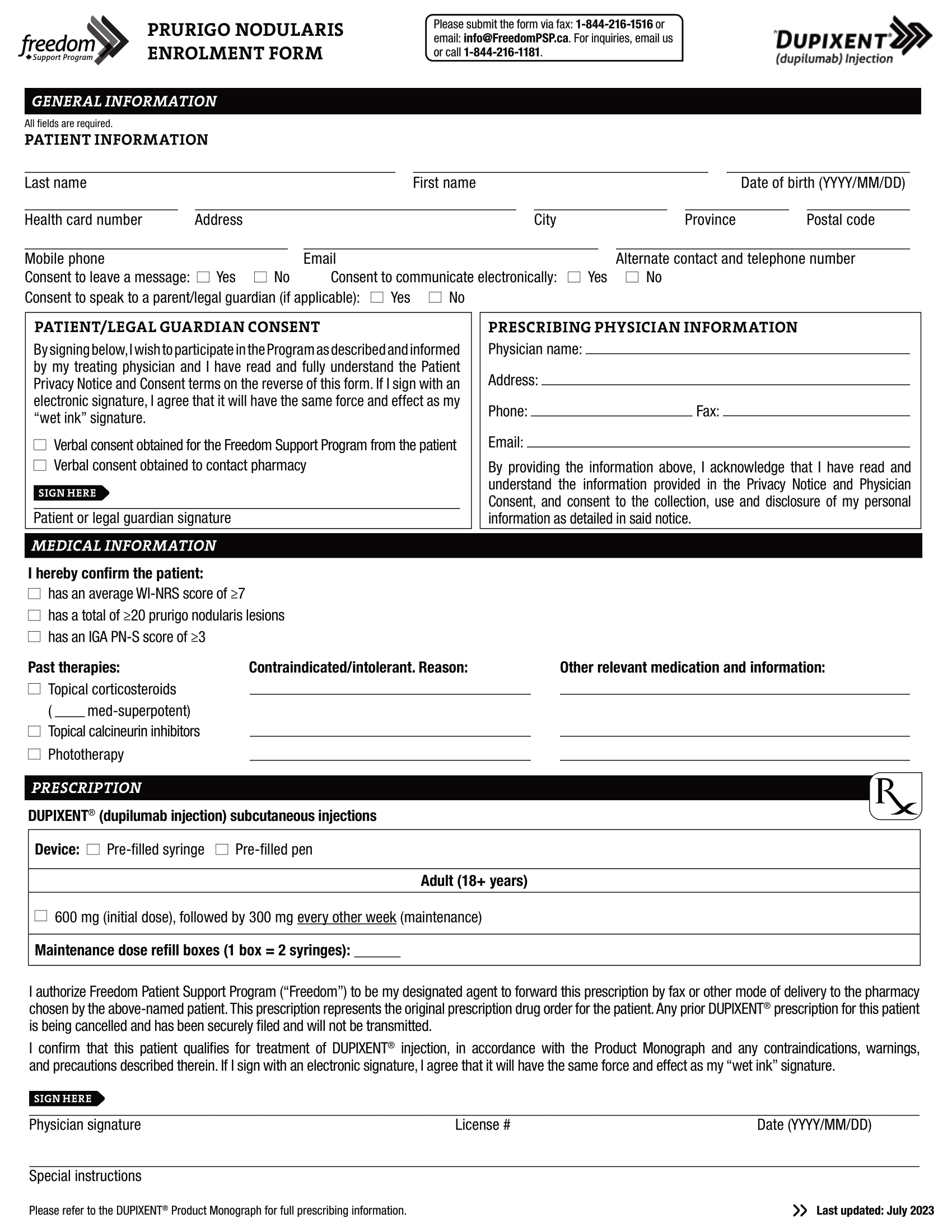
Dupixent (dupilumab) PSP PN Enrolment Form EN 2023 World EMR
Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support program and start. Please provide us with your email address to receive email communications. Choose the appropriate form below and complete the required fields. If i am completing section 5b, i authorize.
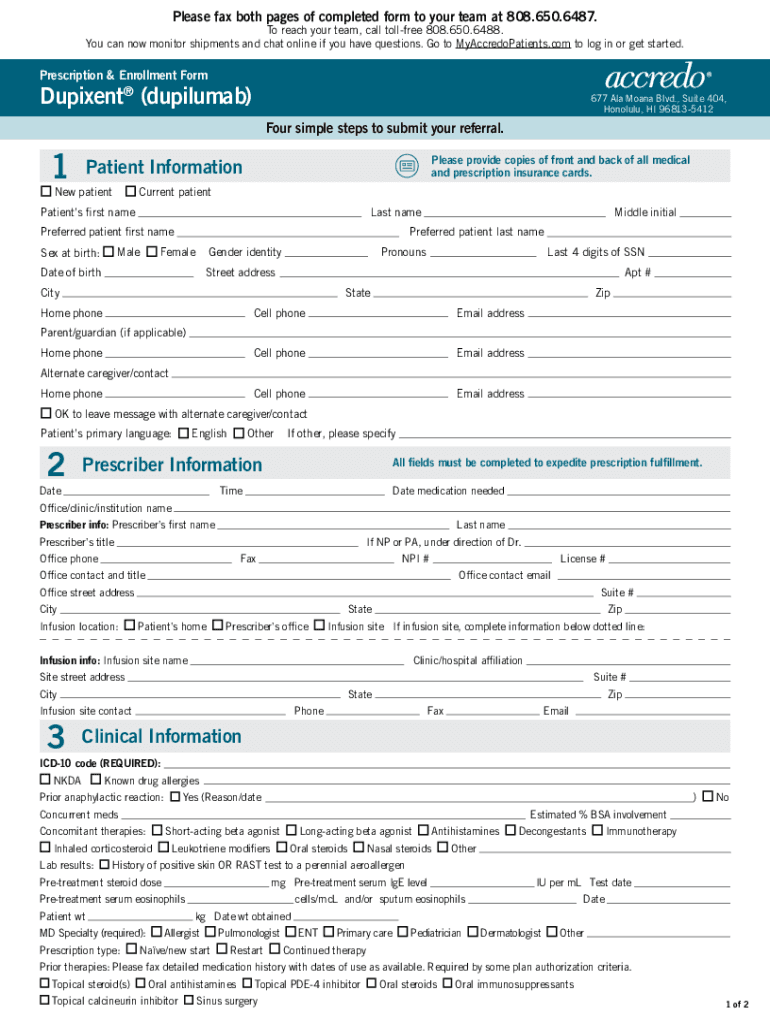
Fillable Online Dupixent (dupilumab) Hawaii. Prescription
Please provide us with your email address to receive email communications. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Choose the appropriate form below and complete the required fields. Start your dupixent treatment with the myway enrollment form. Patients, prescribers, and specialty pharmacies require the dupixent enrollment.
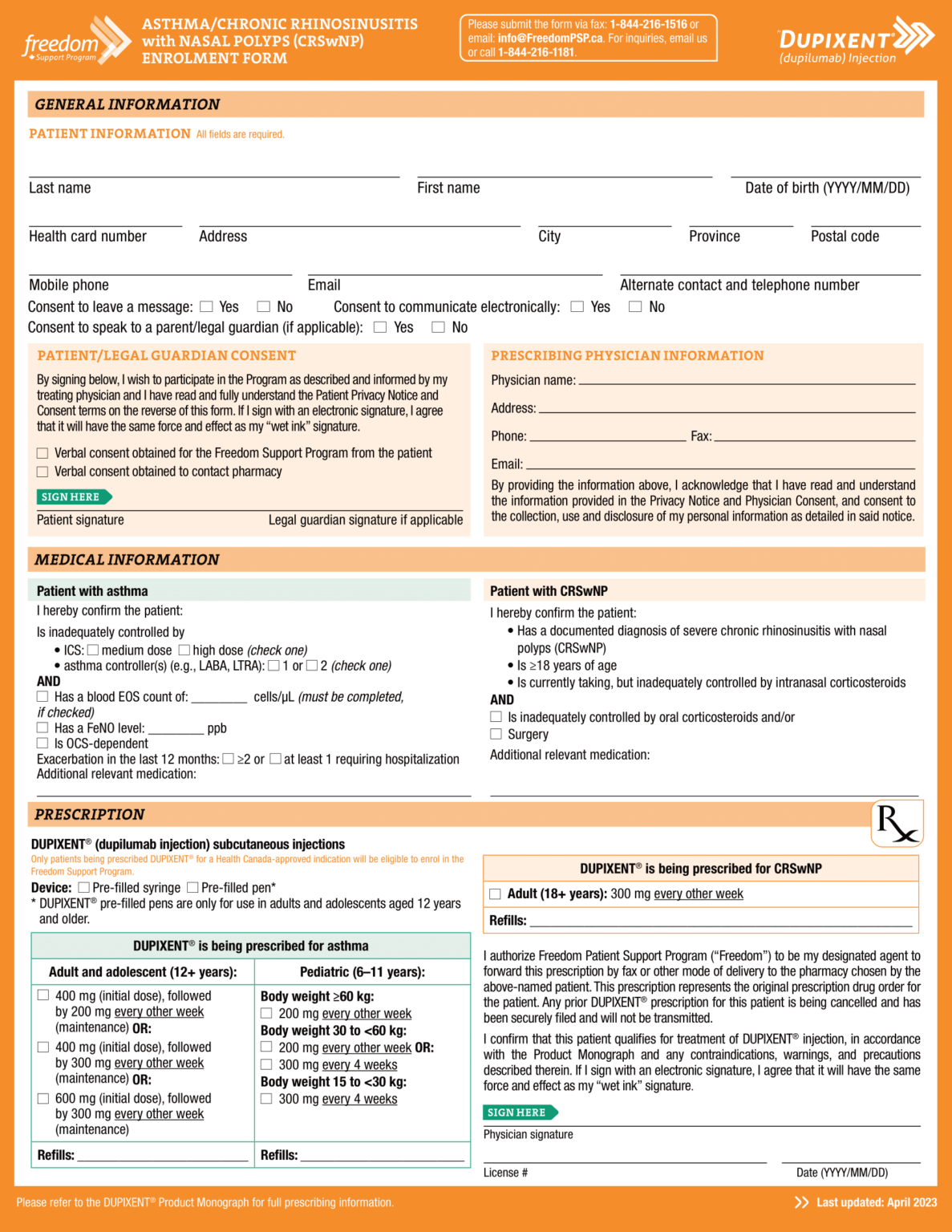
Dupixent (dupilumab) PSP Enrolment Form Asthma CRSwNP EN 2023 World EMR
Start your dupixent treatment with the myway enrollment form. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Please provide us with your email address to receive email communications. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. If i am completing section 5b, i.

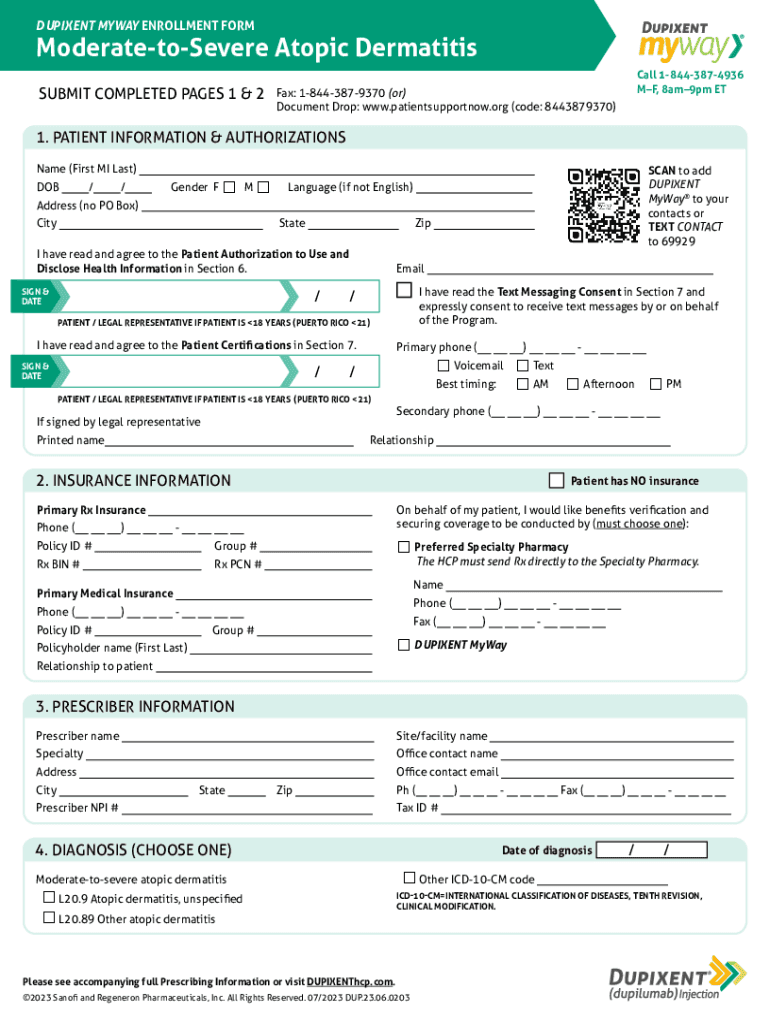
Dupixent (dupilumab) PSP Atopic Derm Enrolment Form CA EN 2023 World
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Please provide us with your email address to receive email communications. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Patients, prescribers, and specialty.

Dupixent Enrollment Form Fill Online, Printable, Fillable, Blank
Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. Please provide us with your email address to receive email communications. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support.

Dupixent Enrollment Form 20202022 Fill and Sign Printable Template
Choose the appropriate form below and complete the required fields. Please provide us with your email address to receive email communications. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. If i am completing section 5b, i authorize for my commercially insured patient one or more months of.

Fillable Online Enrollment Form Dupixent Fax Email Print pdfFiller
Please provide us with your email address to receive email communications. Dupixent myway is a patient support program that can help your patients access dupixent and find support throughout their treatment journey. Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support program and start. Choose the appropriate form below and complete the required.
Fillable Online DUPIXENT MYWAY ENROLLMENT FORM Fax Email Print pdfFiller
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. Choose the appropriate form below and complete the required fields. Dupixent myway is a patient support program that can help your patients access dupixent.
Start Your Dupixent Treatment With The Myway Enrollment Form.
Please provide us with your email address to receive email communications. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Free fillable pdf for patients with eczema, asthma, nasal polyps, and more. Choose the appropriate form below and complete the required fields.
Dupixent Myway Is A Patient Support Program That Can Help Your Patients Access Dupixent And Find Support Throughout Their Treatment Journey.
Patients, prescribers, and specialty pharmacies require the dupixent enrollment form to initiate enrollment in the support program and start.