Cigna Provider Appeal Form Pdf - Please complete the below form. Fields with an asterisk ( * ) are required. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. Be specific when completing the description of dispute and.
Fields with an asterisk ( * ) are required. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Be specific when completing the description of dispute and. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. Please complete the below form. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing.
Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Please complete the below form. Be specific when completing the description of dispute and. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing. Fields with an asterisk ( * ) are required. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal.
Fillable Online BRequestb for Appeal or Reconsideration Cigna Fax
Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Fields with an asterisk ( * ) are required. Please complete the below form. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing. The form will help.
Fillable Online Cigna Medicare Advantage Arizona Non Ccontracted
The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Be specific when completing the description of dispute and. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Please complete the below form. Fields with.
Fillable Online Cigna Medicare Advantage Member And Representative
The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing. This completed form and/or an appeal letter requesting an appeal review and.

medicalreimbursementclaimform PDF Cigna Receipt
This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. Please complete the below form. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Log in to cignaforhcp.com to find the dental.
Fillable Online medicaid nv MAC Pricing Appeal Form Providers Cigna
Be specific when completing the description of dispute and. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing. Fields with an.
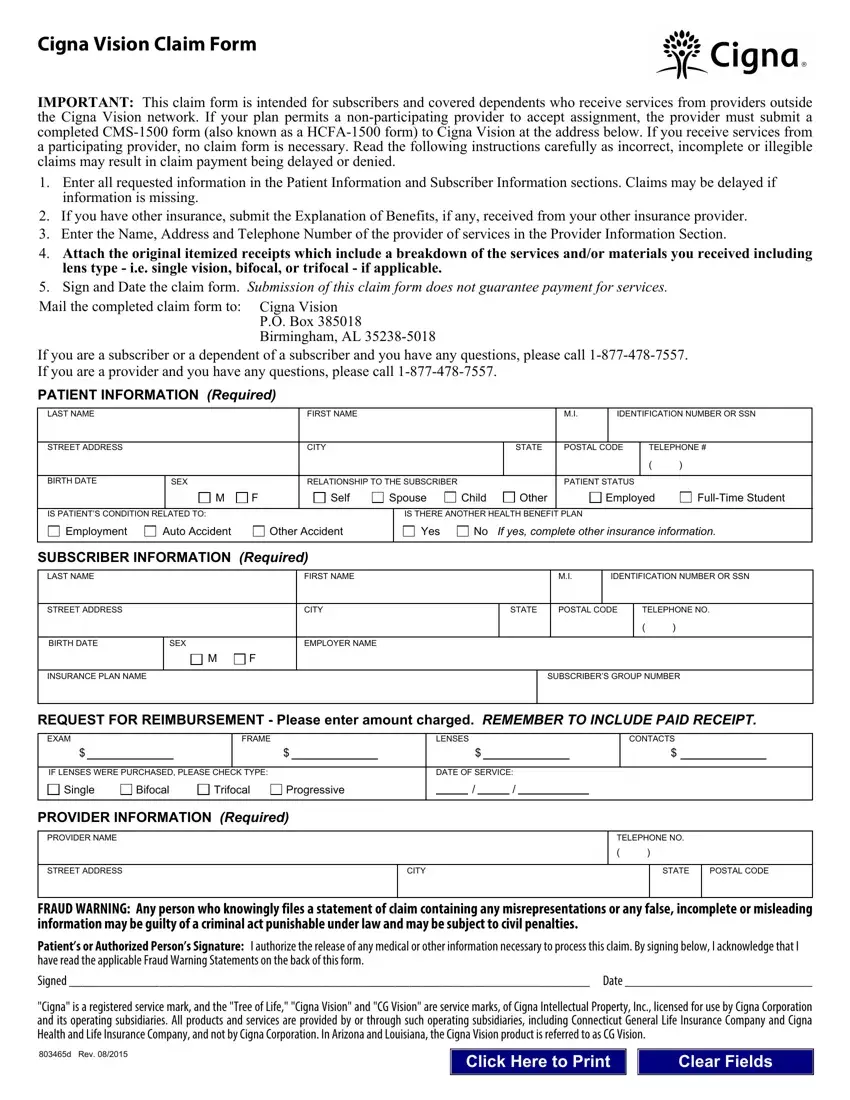
Cigna Vision Claim Form ≡ Fill Out Printable PDF Forms Online
Please complete the below form. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. Fields with an asterisk ( * ) are required. Be specific when completing the description of dispute and. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with.

Fillable Online CIGNA HEALTHCARE FOR SENIORS ELECTION OF APPEAL PROCESS
Be specific when completing the description of dispute and. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Please complete the below form. Log in.
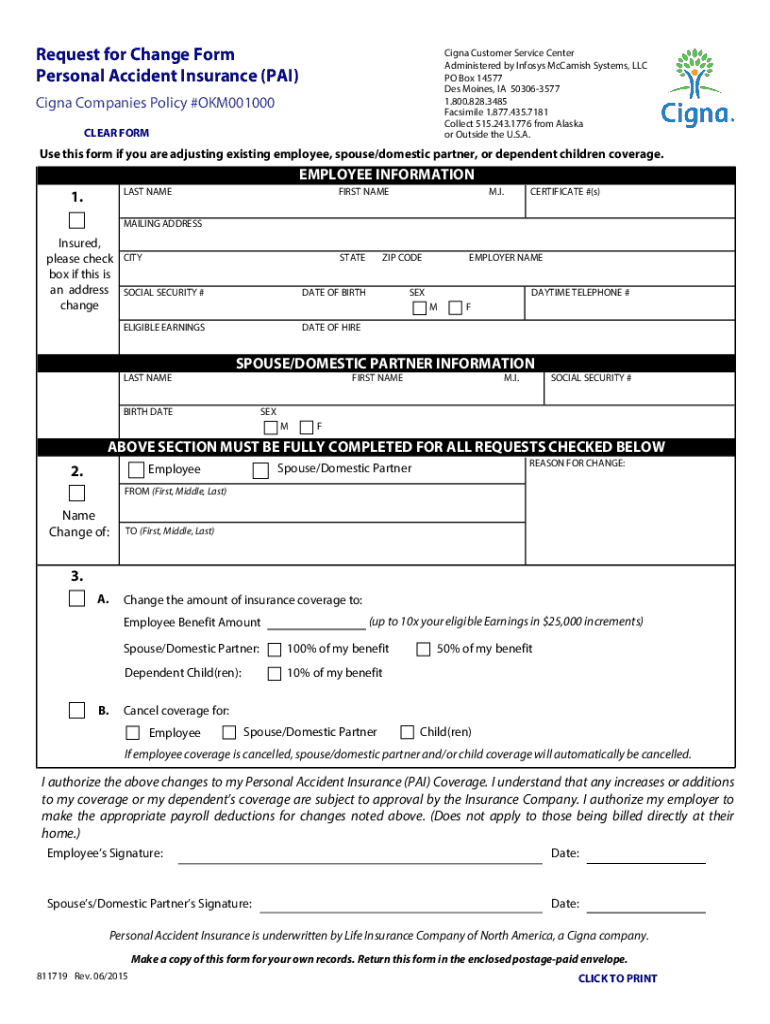
Fillable Online Cigna Companies PAI Request For Change. 811719
This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Fields with an asterisk ( * ) are required. Please complete the below.

Cigna HealthSpring Request for Appeal
Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Please complete the below form. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is. Fields with an asterisk ( * ) are required. The form will help to.
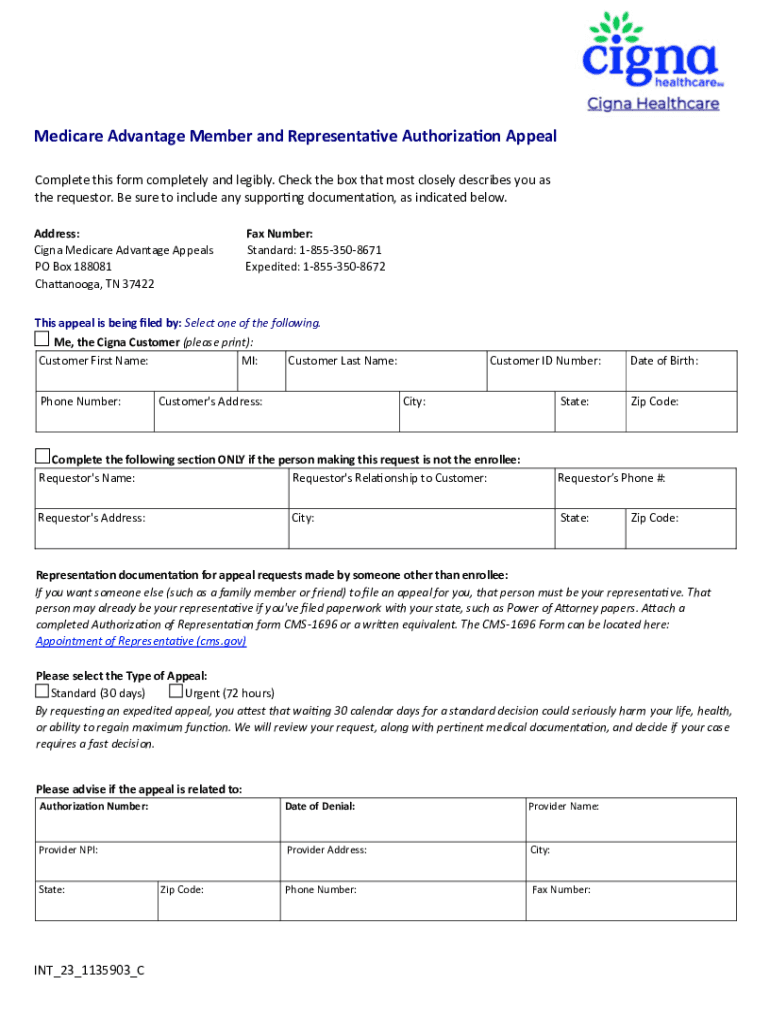
Fillable Online Cigna Medicare Advantage Member And Representative
Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Please complete the below form. Fields with an asterisk ( * ) are required. Be specific when completing.
The Form Will Help To Fully Document The Circumstances Around The Appeal Request And Will Also Help To Ensure A Timely Review Of The Appeal.
Fields with an asterisk ( * ) are required. Please complete the below form. Quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing.
Be Specific When Completing The Description Of Dispute And.
This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is.