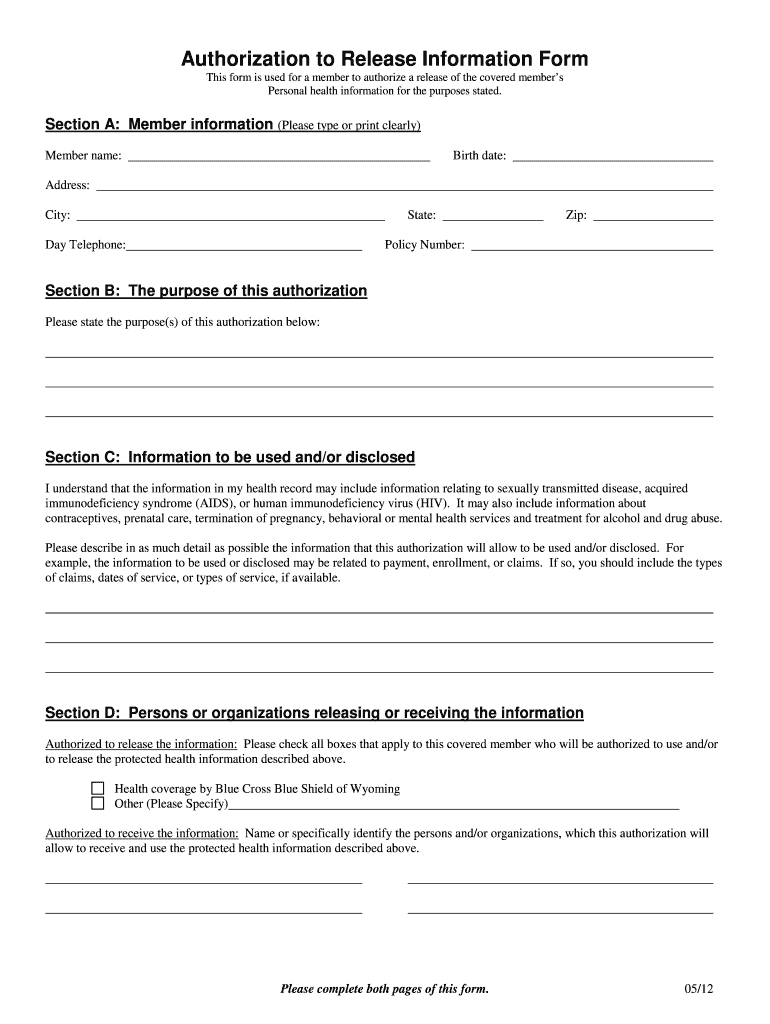
Authorization To Release Information Form - This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. Complete all sections of this authorization as appropriate to your request. Provide a copy of my health information to me. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record.
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Complete all sections of this authorization as appropriate to your request. Provide a copy of my health information to me. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record.
Provide a copy of my health information to me. Complete all sections of this authorization as appropriate to your request. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family.
FREE 10+ Sample Employee Information Forms in PDF MS Word
Provide a copy of my health information to me. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Complete all sections of this authorization as appropriate to your request. To allow.
Consent To Release Information Form
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Provide a copy of my health information to me. Complete all sections of this authorization as appropriate to your request. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. To allow.
FREE 14+ Release Authorization Forms in PDF MS Word Excel
To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. Complete all sections of this authorization as appropriate to your request. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. This form is to be used by a patient or legal representative to authorize the release of.
Fillable Online Letter of authorization to release information. Sample
Provide a copy of my health information to me. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Complete all sections of this authorization as appropriate to your request. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. To allow.
Authorization to Release Information Form Fill Out and Sign Printable
Provide a copy of my health information to me. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Complete all sections of this.
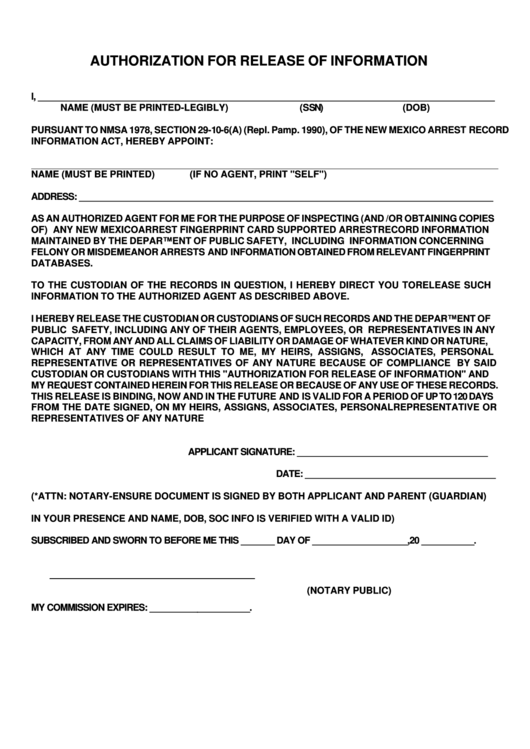
Authorization For Release Of Information Form Printable Pdf Download
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Provide a copy of my health information to me. Complete all sections of this authorization as appropriate to your request. To allow.

SAMPLE AUTHORIZATION TO RELEASE INFORMATION TEMPLATE FORM
Complete all sections of this authorization as appropriate to your request. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. Provide a copy of my health information to me. This form is to be used by a.

Printable Blank Authorization To Release Information Form
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Provide a copy of my health information to me. Complete all sections of this authorization as appropriate to your request. To allow.

Authorization To Release Information Form Word PDF Google Docs
Complete all sections of this authorization as appropriate to your request. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Provide a copy of my health information to me. To allow.

Release Of Information Forms Printable (BLANK TEMPLATE)
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. Provide a copy of my health information to me. This form is to be used by a patient or legal representative to authorize the release of information to.
This Form Is To Be Used By A Patient Or Legal Representative To Authorize The Release Of Information To A Third Party (Other Than A Family.
To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. Complete all sections of this authorization as appropriate to your request. Provide a copy of my health information to me. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record.