Arikayce Enrollment Form - Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. This form is intended for patients enrolling in the inlighten patient support program for arikayce, a medication for treating mycobacterium avium. Get “extra help” with prescription medicine costs. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Enroll before the plan year or at any month during the year by contacting your medicare part d plan.
The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. This form is intended for patients enrolling in the inlighten patient support program for arikayce, a medication for treating mycobacterium avium. Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Get “extra help” with prescription medicine costs.
This form is intended for patients enrolling in the inlighten patient support program for arikayce, a medication for treating mycobacterium avium. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Get “extra help” with prescription medicine costs.
Editable Student Form Templates in Word to Download
Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Enroll before the plan year or at any month during the year by contacting your medicare part.

Owwa Enrollment Form For Domestic Workers PDF Labor
Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Get “extra help” with prescription medicine costs. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Patient support program enrollment consent agree to enroll in the inlighten patient.

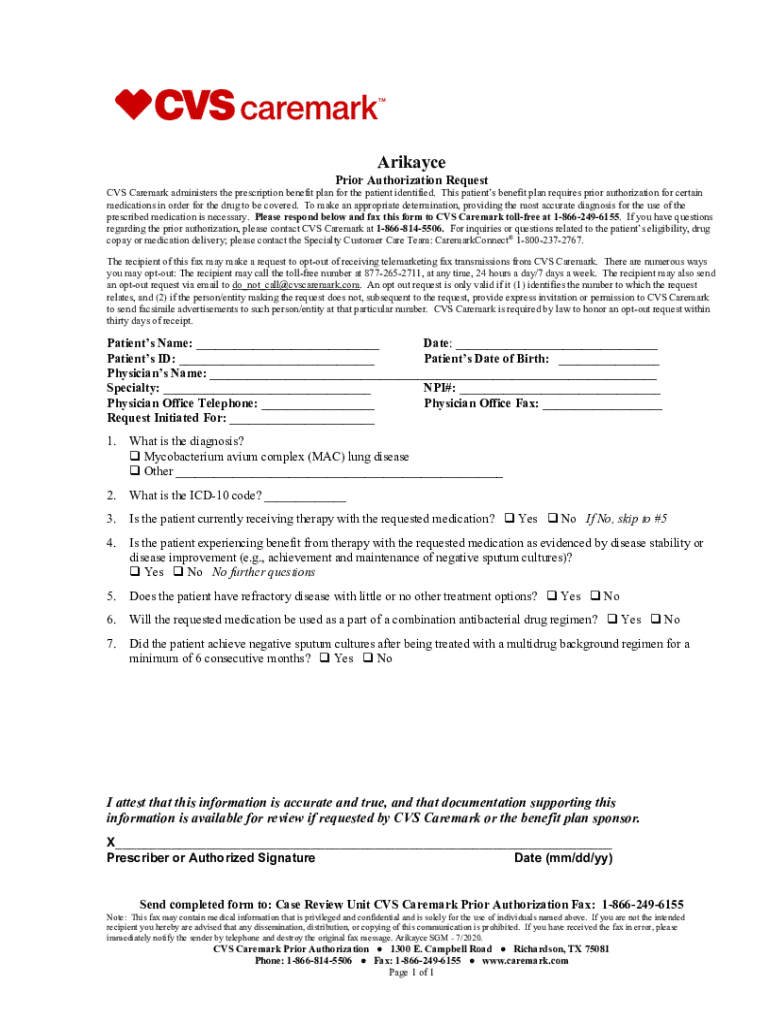
Prescribing ARIKAYCE (amikacin liposome inhalation suspension)
Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. This form is intended for patients enrolling in the inlighten patient support program for arikayce, a medication for treating mycobacterium avium. Enroll before the plan year or at any month during the year by contacting your medicare part d.
Fillable Online Arikayce Web. Arikayce Web Fax Email Print pdfFiller
Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify.
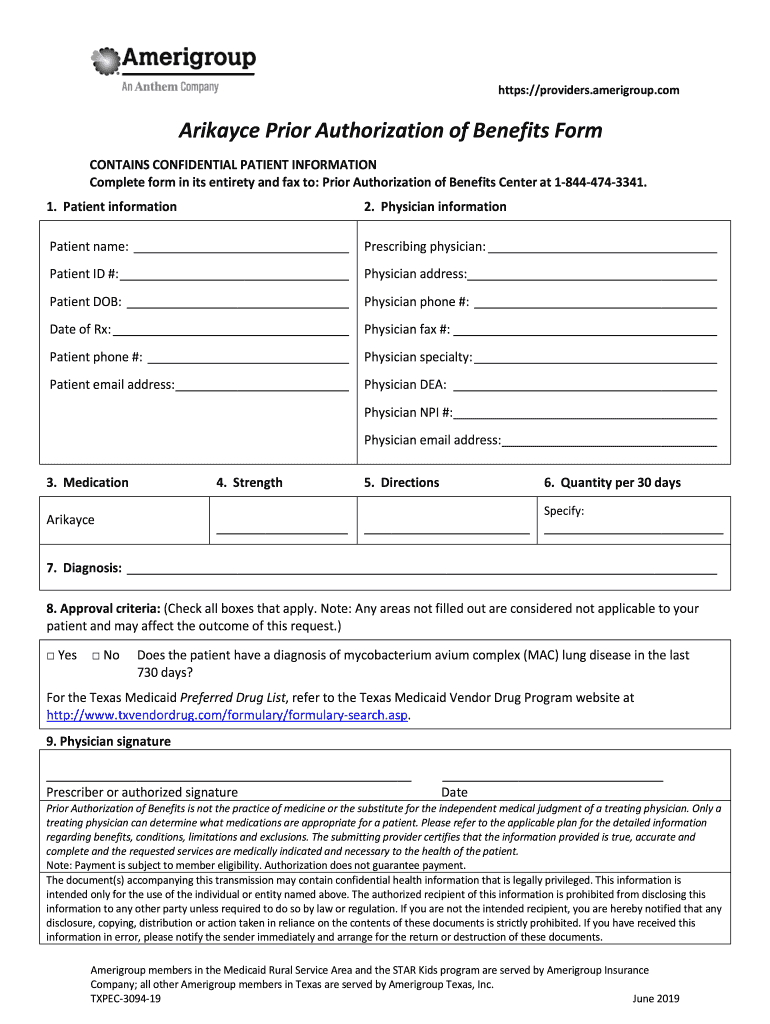
Fillable Online Arikayce Prior Authorization of Benefits Form Fax Email
The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. This form is intended for patients enrolling in the inlighten patient support program for arikayce, a medication for treating mycobacterium avium. Get “extra help” with prescription medicine costs. Patient support program enrollment consent agree to enroll in the inlighten patient.
Taking ARIKAYCE® ARIKAYCE® (amikacin liposome inhalation suspension)
This form is intended for patients enrolling in the inlighten patient support program for arikayce, a medication for treating mycobacterium avium. The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. Enroll before the plan year or at any month during the year by contacting your medicare part d plan..
Simple Green Enrollment Forms Venngage
Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. Get “extra help” with prescription medicine costs. This form is intended for patients enrolling in the inlighten patient support program.

Preschool Admission Form Template 123FormBuilder
The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the..
Daycare Enrollment Forms, Fully Editable, Child Care Enrollment Forms
The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Enroll before the plan year or at any month during the year by contacting your medicare part d.
DIY Child Care Enrollment Form, Editable, Canva Template, Personalized
Enroll before the plan year or at any month during the year by contacting your medicare part d plan. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify.
This Form Is Intended For Patients Enrolling In The Inlighten Patient Support Program For Arikayce, A Medication For Treating Mycobacterium Avium.
Patient support program enrollment consent agree to enroll in the inlighten patient support program provided by insmed and verify that the. Program enrollment—by signing below, i agree to enroll in the arikares support program and verify that the information in the “patient information”. The inlighten enrollment form allows you to prescribe arikayce and your patients to enroll in the inlighten patient support program. Get “extra help” with prescription medicine costs.