Ambetter Appeal Form - Learn more about the procedures. So, to make working with us easier, we developed the ambetter provider toolkit. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. If you do not have access to a phone, you can complete. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. It’s designed to provide you with valuable education and materials.
It’s designed to provide you with valuable education and materials. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. Learn more about the procedures. If you do not have access to a phone, you can complete. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. So, to make working with us easier, we developed the ambetter provider toolkit.
Learn more about the procedures. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. So, to make working with us easier, we developed the ambetter provider toolkit. If you do not have access to a phone, you can complete. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. It’s designed to provide you with valuable education and materials.
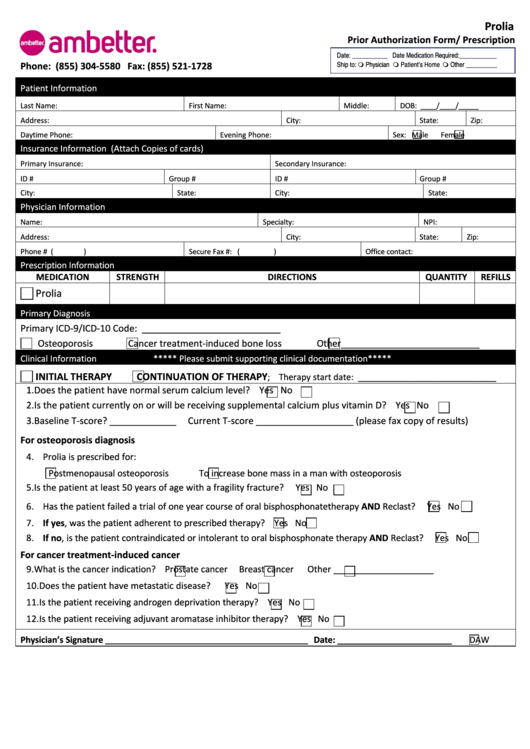
Ambetter Prior Authorization Form Florida Fill Out Si vrogue.co
A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. So, to make working with us easier, we developed the ambetter provider toolkit. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. If you do not have.

Fillable Online Ambetter Health Authorized Representative Designation
Learn more about the procedures. If you do not have access to a phone, you can complete. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. So, to make working with us easier, we developed the ambetter provider toolkit. It’s designed to provide you with valuable education and.
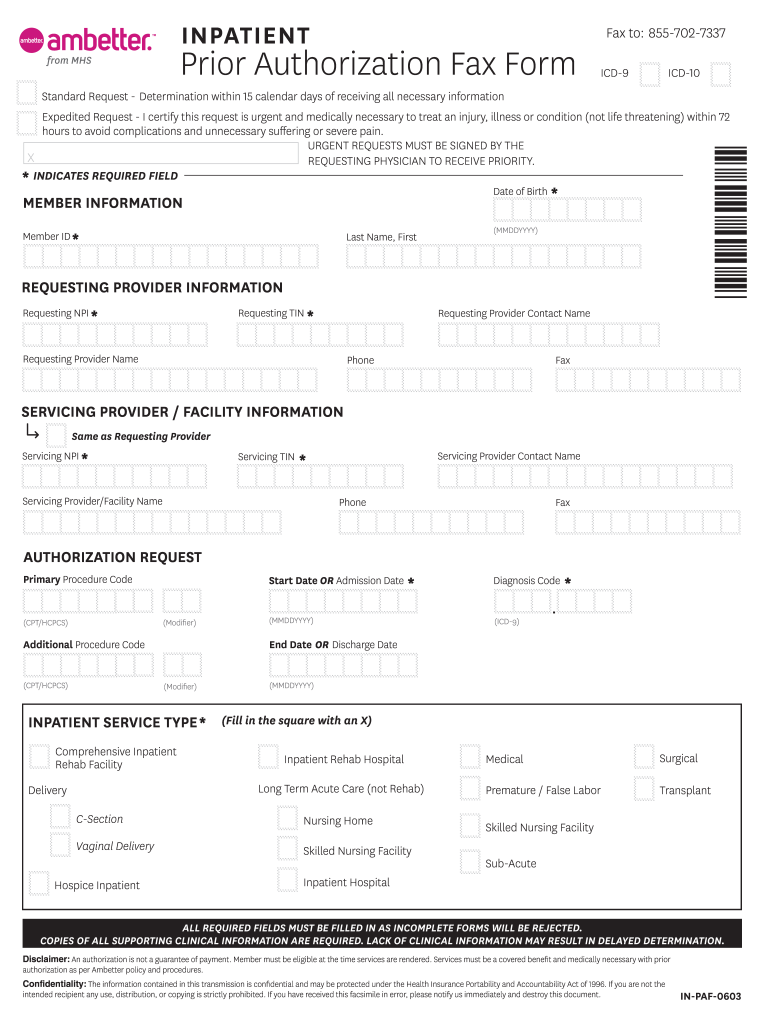
Inpatient Form Ambetter Fill Online, Printable, Fillable, Blank
It’s designed to provide you with valuable education and materials. So, to make working with us easier, we developed the ambetter provider toolkit. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. Learn more about the procedures. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally.
Ambetter Inpatient Prior Authorization PDF Form FormsPal
It’s designed to provide you with valuable education and materials. If you do not have access to a phone, you can complete. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. A member has.
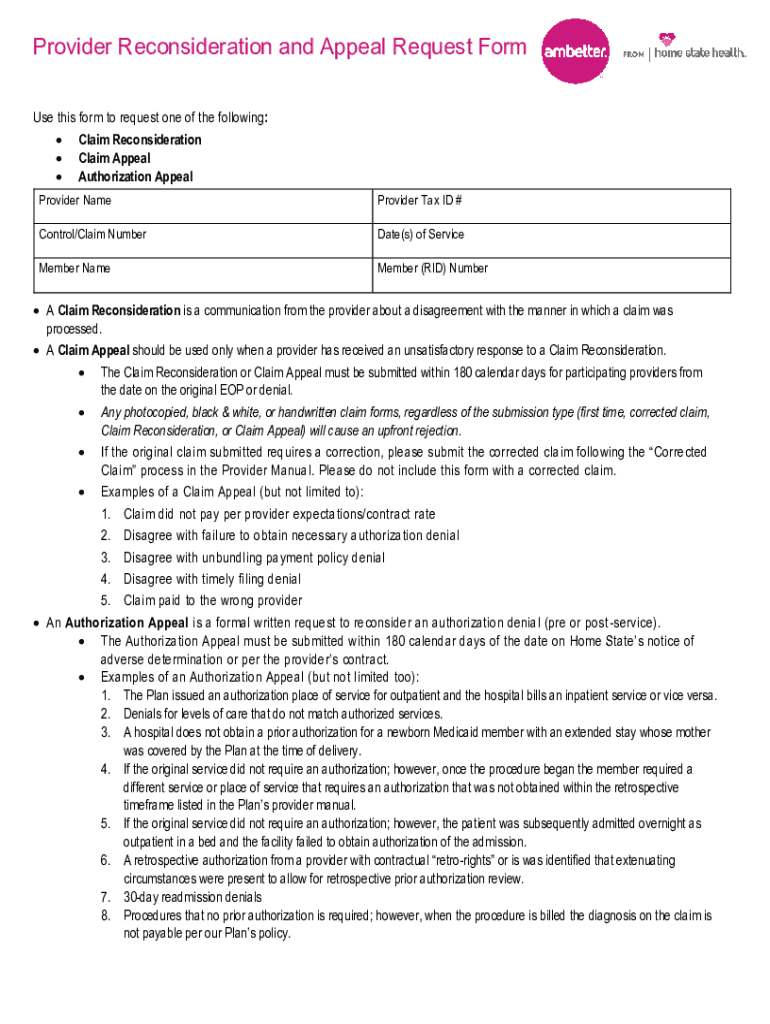
Fillable Online Ambetter MO Provider Reconsideration and Appeal
It’s designed to provide you with valuable education and materials. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. Provider request for reconsideration and claim dispute form use this form as part of the.

Fillable Online Ambetter Out of Network Request Form. Out of Network
A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. So, to make working with us easier, we developed the ambetter provider toolkit. Learn more about the procedures. It’s designed to provide you with valuable.

How to Cancel Ambetter Insurance?(A StepbyStep Guide)
A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. Provider request for reconsideration and claim dispute form use this form as part of the ambetter from superior healthplan request for. It’s designed to provide you with valuable education and materials. All ambetter from coordinated care members are entitled.

Fillable Online KY AMB Provider Request for Reconsideration and
All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. So, to make working with us easier, we developed the ambetter provider toolkit. It’s designed to provide you with valuable education and materials. Learn more.

Fillable Online Ambetter from MHS Psychological OR Neuropsych Testing
All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. It’s designed to provide you with valuable education and materials. If you do not have access to a phone, you can complete. Learn more about the procedures. So, to make working with us easier, we developed the ambetter provider toolkit.
Fillable Online Appeal or Grievance Form Ambetter from Health Net Fax
So, to make working with us easier, we developed the ambetter provider toolkit. If you do not have access to a phone, you can complete. Learn more about the procedures. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. It’s designed to provide you with valuable education and.
Provider Request For Reconsideration And Claim Dispute Form Use This Form As Part Of The Ambetter From Superior Healthplan Request For.
Learn more about the procedures. A member has 180 calendar days from ambetter's notice of adverse determination to file an appeal, either orally or in writing. All ambetter from coordinated care members are entitled to a complaint/grievance and appeals process. So, to make working with us easier, we developed the ambetter provider toolkit.
It’s Designed To Provide You With Valuable Education And Materials.
If you do not have access to a phone, you can complete.